Faces
of covid

Faces
of covid
COVID-19 - a global experience, which spared no one on the planet. Everybody has a memory to share, a story to tell. During the pandemic a lot of people felt grief, fear or helplessness. Luckily, many also had help, thanks to dedicated individuals, organizations or governments.
Among others, the Netherland Red Cross also responded to the global crisis. In partnership with nine National Red Cross Societies, the Netherland Red Cross supported projects in different African and Middle-Eastern countries, reaching millions of people in need. The programme was funded by the Dutch Ministry of Foreign Affairs (MoFA) and individual donations of Dutch public. As the pandemic evolved, over time these projects’ focus also changed. In the early days the main aim was to prevent the transmission of the novel virus. Seeing the growing need for correct, trustworthy information, thousands of Red Cross and Red Crescent (RCRC) volunteers were mobilized to pass on that information, collect feedback from community members, and promote protective behaviors. Later, as the deeper consequences of lock-down and isolation measures began to appear, the emphasis shifted to dealing with the socio-economic effects of the pandemic. Vulnerable families faced dire financial situations - and they needed not just material, but emotional and mental support. Offering emotional support to health staff and RCRC volunteers who suffered from fatigue and exhaustion at that stage became central to the projects. During the last phase, the project activities centered mainly around promoting and facilitating the COVID-19 vaccine - convincing people to get vaccinated and advocating for widespread access.
In this online report, we provide insights into the various project activities and how they affected people's lives. We will introduce you to people, the faces of COVID, who needed or provided help.

Tap for more information

PROJECT
COUNTRIES
The “COVID-19 response programme” supported different projects and activities in 9 countries. (2020-2022)*
*the programme had different sources of funding, mainly from the Dutch Ministry of Foreign Affairs (MoFA) and individual donations of Dutch public
VOLUNTEERS
VOLUNTEERS
the community really depended on the information provided by the Red Cross volunteers
When people face an unknown, terrifying and never-experienced situation, probably the most valued thing is accessing the right information. Even after the first cases of COVID-19 appeared, communities still had very limited or deficient knowledge about the virus - how it spreads, how it affects the body, how to prevent it. Later, too much information caused problems as misinformation began to flood everyday conversations. In providing the correct facts and guiding people toward the right protective behaviors, the Red Cross volunteers played a critical role. As one of the Red Cross staff members said: “the volunteers were the backbone of the projects, they were at the forefront of the response”.
Despite all of the personal challenges they went through, volunteers provided their service voluntarily, and happily. As the carriers of often inconvenient facts or hard to follow advice, they often had to deal with the resistance, anger and fear of the communities. They also had to cope with the everyday stress of the possibility of getting infected and bringing the disease home to their own families. At the very beginning of the pandemic, they had to work without proper protective equipment as masks, gloves and aprons were simply not available in the market.
Where the main source of news was fellow neighbors or often confusing social media, it is volunteers who became the trusted source of information. Going door to door, providing household visits or sitting down with community members, the Red Cross volunteers managed to reach many people, especially in rural areas. In Ivory Coast, for example, the volunteers reached almost 20.000 community members in the first months of response through group talks and hand washing demonstrations. Volunteers also distributed different useful items, like face masks, sanitizers or soap bars.
When the health facilities were overloaded, volunteers helped with screening efforts, measuring temperatures or doing registrations. They also boosted the confidence of the community to access health care, when mothers would be fearful to bring their children to the facilities, ensuring continuation of regular health services. There were places where they even mobilized communities to donate blood, as regular donors got scared of health facilities, and blood became a scarce resource. Publicly taking up vaccines, volunteers also served as role models to encourage communities to get vaccinated. Thanks to their special training, volunteers were also able to give psychosocial support to help people cope with their fears and anxieties. In Zambia they wrote songs and poems to encourage the affected frontline workers, but they also contributed in drama plays to make the messages more accessible to communities.
The Red Cross helped their own volunteers in many ways. Besides the several training sessions they received to deepen their knowledge and strengthen their confidence, with the involvement of professional psychologists, they got regular mental health support too and received proper protection gear when this became available. Listening to their fears and concerns, supporting, encouraging and reassuring them as often as possible, the Red Cross staff also did their very best to assist their volunteers. In Ethiopia the project ensured that all volunteers engaged in the COVID-19 project had appropriate insurance.
In Ethiopia, Sudan, Zambia and Ivory Coast, a total of 2714 volunteers were trained and mobilized to support COVID-19 community actions. In Haiti, Benin and the Central African Republic, the training of volunteers was followed by the training of trainers (TOT) approach. Using this method, a larger number of people got trained in a shorter time.
COVID19 related health topics and personal safety
Infection prevention, control and contact tracing, plus usage of personal protection equipment (PPE)
CEA
Community Engagement and Accountability
CBHFA
Community Based Health and First Aid
PFA/MHPSS
Psychological First Aid, Mental Health and Psycho Social Support (Self care)
RCCE
Risk Communication and Community Engagement
PGI
Protection, Gender, Inclusion
WASH
Water, Sanitation and Hygiene Promotion
CVA
Cash and Voucher assistance
Types of volunteer training
(click on the icons to see the different types of trainings)INFLUENCERS
you can pray about it, but you also need to take measures to prevent it
Despite the enormous effort of the volunteers and the messages spread through the different mass communication channels, there was still a need to reach and convince different segments of the population. Supporting the usual awareness raising tools and activities, the projects needed to think innovatively. The role of influential community members in inspiring people to follow certain rules or adapt new behaviors was clear from the beginning. In order to facilitate behavior change the projects involved different influencers.
For example, religious or community leaders were involved in the program in several places. In Benin, 547 mother group members were trained, while in the Central African Republic 320 so-called “sensitizing agents” were brought in. They were instrumental to pass information to their peers.
Convincing the younger generation to wear a protective face mask was a very big challenge in Zambia. Through training, The Zambian Red Cross involved 340 youths as peer educators who participated in radio and TV programs sharing their own testimonies. They also conducted school competitions and other outreach activities. Youth were invited to a webinar where they could discuss not just the pandemic but also the role the youth themselves saw having in the response. To ease the role of peer educators and youth generally, the project printed and distributed 5.000 units of educational material focusing on behavior change related to vaccine uptake, mental health and how to prevent the infection.
In Ethiopia and Zambia religious and community leaders were also involved in project activities. In Ethiopia, for example, 200 religious leaders were trained and 164 mass awareness raising activities were carried out with their involvement. They spoke during forums and in public places, reaching not only their followers. More than 100 religious leaders participated in a 2-day orientation on psycho-social support. The mental help was particularly well appreciated by the communities. They were not just trusted sources of correct information but also positive role models, especially when there was hesitancy in the communities for vaccination.
Tapping into the locally available skills and choosing preferred traditional methods, in Ethiopia a music group was involved in the projects. The “Guna Band” travelled village to village, and through songs, drama and short role-plays they delivered the most important messages at different community gatherings and public places.
*excerpts from the Guna band role-play sessions (Ethiopia)
FAMILIES
FAMILIES
are you going to feed my children?
COVID-19 hit hard the communities, especially those families whose daily livelihoods were threatened by the new restrictions. As a Red Cross staff member in Zambia described, the most challenging part of the whole project was to convince people to stay home. When a family’s main income source is the small merchandise they produce, but they can’t go to the market to sell it, this can have dire consequences. People had to provide food for themselves and their children every day. As one family member desperately stated “I would rather get the COVID than stay at home”. Even buying masks was an expense they could not afford. On top of their struggle, when schools closed down, they had to deal with the additional costs of their children staying at home. In different project locations, the staff helped the communities, especially the vulnerable families, in several ways.
To address the hard socio-economic situation, in Ivory Coast, the project supported 400 vulnerable families for 3 months with unconditional cash transfers. The money was used for food, health care and education as well as restarting economic activities. In Zambia 17.827 bars of soap and more than 60.000 items of personal protection equipment were distributed in the communities. In Ethiopia the project helped with key hygiene and sanitation items, water and food rations and they also opted to provide quality reusable masks instead of disposable ones. In Sudan more than 4.000 bars of soap were distributed. All this material support was reported to have helped families, especially the vulnerable groups to cope with the hardships.
In the beginning of the pandemic, the lack of reliable information resulted in a lot of fear and uncertainties in the communities. As a community member in Ethiopia revealed it in a focus group discussion: “Soon after we heard cases in Addis and Bahir Dar, the community entered in strong fear. The town looks bare. I personally was afraid that everyone in the town would die because even people in the developed countries could not handle it.” Providing mental help was a core element in the country's projects. The so-called Psychosocial Support (PSS) was provided by trained volunteers, project staff and key community influencers. In Ivory Coast a 24/7 hotline was set up with the involvement of professional psychologists. During the project, 19 Ivorian community groups received PSS.
Supporting the different awareness raising activities, community clean up events, sensitisation campaigns and hand-washing demonstrations were also organized. In Ethiopia, 244 handwashing facilities were set up in public places and health facilities benefiting more than 20.000 community members. In Ivory Coast 356 handwashing facilities were installed and the access to adequate water was enhanced by rehabilitation of 9 water points.
*excerpts from Zambian short documentaries
PATIENTS
they missed their follow up in fear of the pandemic
Although during the implementation of the projects the main challenge was COVID-19 itself, other health problems were also present and made the situation more difficult. Communities had to deal with malaria, polio, or pneumonia, get vaccines for their babies and pregnant mothers needed their routine check-ups.
Due to fear of the pandemic, a significant number of community members missed their medical follow-up appointments. Some others stayed at home sick while developing a disease due to fear of getting COVID-19 in the health facilities. People suffering from non-communicable diseases were experiencing preventable complications due to lack of access to health care for extended time periods. Trained community volunteers helped these patients in many ways. In Ethiopia, for example, they supported people with chronic diseases on their follow-up. Strengthening COVID-19 triage at the health facilities by trained health staff, as well as screening for temperature by trained volunteers, boosted the confidence of the community to access health care and reduced fear of COVID-19 infection at the health facilities.
The majority of the project's activities focused on preventing the spread of COVID-19, while other activities targeted suspected cases and their contacts. In Ivory Coast the project supported setting up a community-based identification and referral of suspected cases, and also supported contact tracing through a team of 29 trained volunteers who were working under the local health workers’ supervision. Volunteers provided COVID-19 information to the identified contacts as well as assured that the contact observed two-week home quarantine measures. In Zambia trained volunteers assisted in contact tracing, identifying thousands of contacts and referring almost one thousand suspected cases to health facilities. In the second phase of the project 7.856 contacts were followed up by the trained volunteers. Volunteers also helped with community follow ups of asymptomatic patients who were isolated at home. Three districts received personal protective equipment in isolation centers.
In Ethiopia psychosocial support (PSS) was provided in quarantine centers to patients and their families and for patients who were in home self-quarantine. All in all, 1.400 individuals received PSS in these facilities. To avoid stigmatization of patients and their families in Zambia, the project conducted a 5-day campaign to tackle stigma and discrimination, reaching more than 30.000 people.
In Palestine the project covered hospital treatment bills and running costs for hospitals and community centers, such as cleaning and catering contract costs. This contribution allowed continuation of urgent and lifesaving hospital services such as dialysis and surgeries.
After vaccines started to be available, the focus moved to awareness raising about COVID-19 vaccines. The important role of religious and community leaders in the project as positive influencers and role models was highlighted by the Red Cross staff, especially when there was strong vaccine hesitancy in the communities. There were various reasons for not taking the vaccine, for example fear of side-effects, not being sure who is eligible, if the vaccine was free of charge, and concerns about the speed at which the vaccine was brought to the market. The Red Cross’ engagement of influencers helped in providing correct and trusted information about the vaccines. Personal testimonies and Red Cross staff and volunteers together with health staff publicly taking up vaccines were also encouraged and increased its uptake.
In Ethiopia a study was done on the wellbeing of the participants during COVID-19.
(click on the circle to see the results)
of the respondents felt a feeling of severe desperation, hopelessness or loneliness.
The major sources of help these people were looking for:
Volunteers
workers
healers
CHILDREN
it affects their mental health, the way they think, the way they grow up
Everybody went through different challenges during the pandemic, but probably children were amongst the biggest victims of COVID-19. With the disruption in their education and their social development, with the missed important childhood vaccinations, the anxiety - the pandemic, directly or indirectly caused a lot of damage in the lives of young ones.
To ease their fears, in Zambia the project provided support to children and encouraged them to express their feelings through story writing, drawing and painting. Branded, colorful masks were distributed and a Corona Virus board game was also developed. To deliver important messages in a child friendly way, a sticker book was designed, produced and distributed. During the project, 120.000 child and youth friendly materials were produced. The project also included abuse and child protection sessions in the volunteer training. Seeing their isolation, Zambian volunteers often organized outdoor games and activities for children.
Besides mental health issues, other health problems also appeared. Due to fears of catching the virus in health centers, a lot of parents missed the immunizations of their children. Many preventable childhood illnesses were on the rise due to drops in vaccine coverage. In Ethiopia, trained youth community volunteers advised mothers not to miss their children’s immunization schedule.
In Palestine, 300 recreational kits were distributed to children in camps. In Ethiopia, 24 Red Cross Clubs were established in schools to create awareness about COVID-19 through peer support. In Sudan (jointly with the Ministry of Education) 16 school examination centers were sanitized and provided with necessary PPE and first aid kits to support 1.726 primary and secondary school students to sit their exams.
Schools generally got special attention through water points rehabilitation, school competitions and special awareness raising sessions. The projects, whenever it was possible, expanded their communication channels to reach the younger generations.
Activities with children*



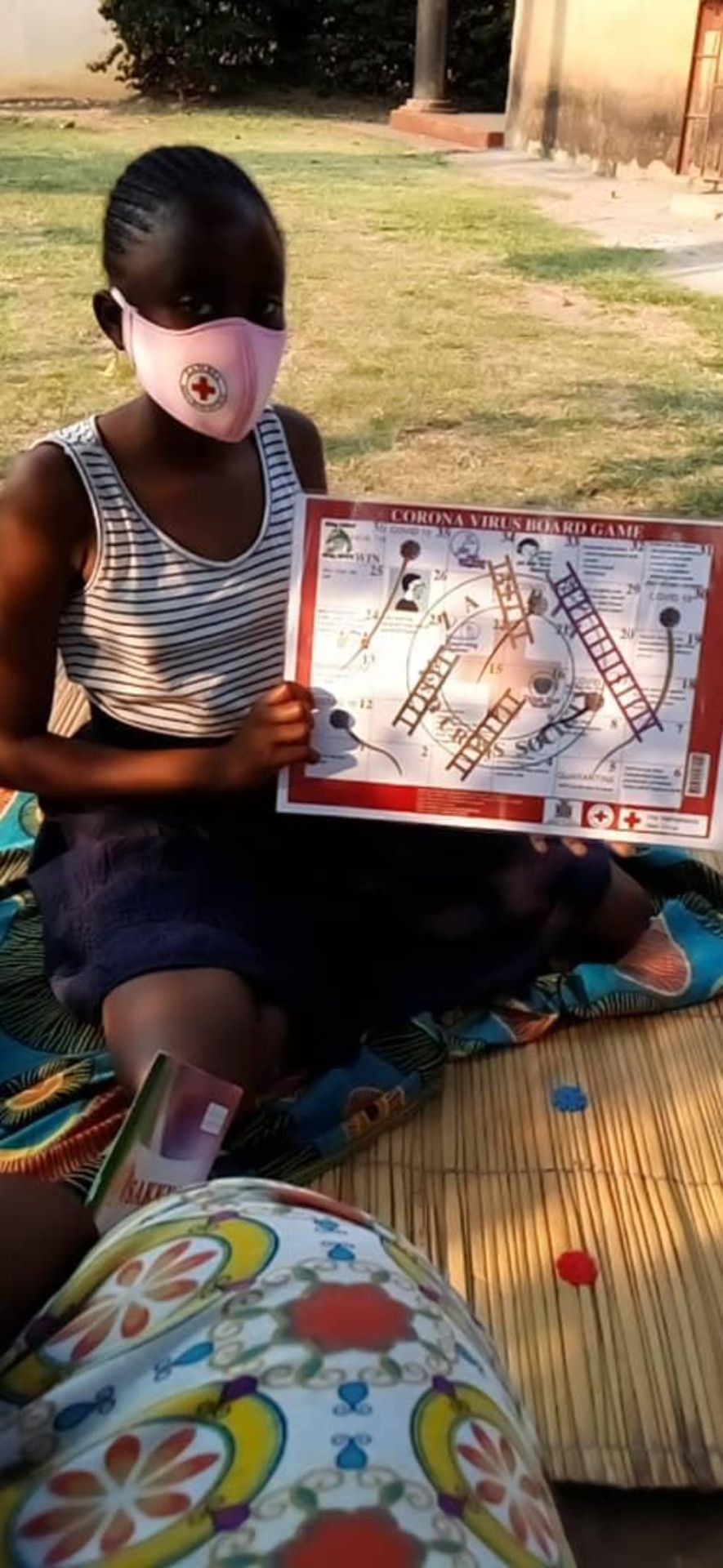
*pictures were taken in Ethiopia and Zambia (© Red Cross)
RED CROSS STAFF

RED CROSS STAFF
the scale was just beyond what we imagined
The COVID-19 pandemic was a never-experienced situation not just for the communities or the governments but for the national Red Cross societies and their staff too. In the very beginning of the pandemic, as one of the staff members described it, there was serious panic - many things happened at the same time and the project staff constantly felt that they were not ready. They were caught between responding to the unknown situation and at the same time managing their own work challenges and safety. A quick response was necessary but there was not enough information or protective equipment. The lack of information in the knowledge about the virus and the pandemic, all caused uncertainties.
Although the Red Cross had the advantage of training or mobilizing volunteers quickly, in the beginning there were not enough volunteers or even staff members. Wider movement restrictions also negatively affected the projects. Staff members had to work from home but a lot of them had no proper internet connection or computer. Not just the meetings, but the training sessions also had to go online or in outdoor places. Meanwhile, steps were taken to rehabilitate the office spaces to comply with social distancing and sanitation requirements.
In Sudan, the Red Cross requested an exemption from the restrictions for its staff and volunteers, which was granted by the government. Later, when an increasing number of project staff and volunteers were getting infected a workforce rotation schedule was introduced.
The pandemic caused high levels of anxiety amongst the volunteers and staff members. The need for psychosocial support and mental health care was highlighted from the beginning of the pandemic as one of the major areas of focus. In all projects significant resources were allocated to training of project volunteers and staff not just on COVID-19 related health topics but about mental health as well. While conducting different activities, the staff personal safety was prioritized, which also eased the stress of getting infected. During the project period, 385 staff and volunteers were insured.
In addition to the pandemic, a lot of countries were affected by multiple crises, so the national Red Cross societies also had to respond to these other emergencies. In Ethiopia there was a major drought, and a locust infestation. In Sudan polio reappeared, and the unprecedented floods increased the incidence of malaria which further strained the already weak health systems.
COVID experiences*
* Selam Seje, Red Cross staff member (Ethiopia)
HEALTH
WORKERS
everyone is fighting silent battles
During the pandemic, the capacity of the health system was stretched to capacity. As a major negative impact, both the access to regular and essential health services, and also the availability of such services, were significantly compromised. Increasing numbers of health workers were getting infected and were unable to work, but even among those who could work there was a strong fear of infection, mainly because of lack of relevant information or proper equipment.
The projects supported the Ministries of Health with case finding, contact tracing or follow-ups with people in self-isolation. In the border area of the Ethiopian Somali region, screening of refugees was conducted by the Red Cross. Reducing the load on the system, different health institutions got material support in the form of personal protective equipment, other infection prevention and control items, and hygiene materials. To lower the financial struggle, in Sudan the project supported 30 health facility staff salaries.
WASH infrastructure was also rehabilitated in several institutions. In Ethiopia, 244 handwashing facilities were set up, a lot of them in health facilities. In Sudan, the project rehabilitated and constructed medical waste management rooms and rehabilitated latrines in primary health care centers. In Ivory Coast, 356 handwashing facilities were installed and 5.053 bars of soap were distributed in communities and health facilities. To lessen the burden on health workers, Red Cross volunteers helped in health facilities and immunization centers, mostly with registration, observing physical distancing or hand sanitizing and also with taking the temperatures of patients.
One of the major challenges was the fear and anxiety of the health workers. As one of the project participants put it: “While of late I have been battling with depression and sometimes am overwhelmed. Being a nurse who worked in a mental health institution I sometimes encourage myself by believing that even a nurse needs a nurse when sick.” Focusing on the mental well-being of the health workers, regular training sessions were provided to them, focusing on not just COVID-related information, but on psychological first aid too. Quoting a health worker from Ethiopia: “Since the pandemic is new to everyone, there was an awareness gap even among health providers. There was a strong fear to give essential healthcare services because of lack of knowledge about the nature of the disease and its prevention mechanisms.”
To ease the stress of the front-line workers, in Zambia the project launched a campaign called “Behind the mask”. The initiative's aim was to bring attention to issues which are a lot of times hidden by the mask. Red Cross volunteers wrote and performed songs and poems to encourage the health workers, to keep their spirits high and remain positive about the future. The following testimony from a Zambian community health worker shows the importance and the positive effect of the mental help: “Thanks a lot for the psychological first aid workshop, it was medicine to my soul. I was crying inside but you showed me some skills on how to control my mood and relax when I am stressed or in distress. Thanks a lot, may God richly bless you.”
Behind the mask
This poem was written by Zambian volunteers (told by Gloria Kunyenga, Red Cross staff member, Zambia)

LESSONS OF
COVID
Way forward for the future
The first two years of the pandemic taught everybody hard lessons, but learning from these experiences can help us to prepare and respond better for future pandemics, epidemics or other emergency situations.
The COVID-19 projects showed clearly that the unique position of the Red Cross was, and can be, a solid base for timely and proper actions in the future. In responding to the situation, the existing network and capacity of volunteers, the good connections the volunteers had with communities, and the already established trust were all crucial elements. Exercising the Red Cross’s auxiliary role by supporting health authorities and keeping strong engagement with local stakeholders, influencers, and communities was also very important.
Ensuring the continuity of business for the staff and volunteers in spite of movement restrictions, physical distance, lack of IT equipment and digital skills and other uncertainties was challenging, but on the institutional side it was necessary to be able to respond to the pandemic. Empowering volunteers with appropriate training, skills, knowledge, and also providing insurance and individual protection equipment also proved to be essential.
The projects also demonstrated that in emergency situations we have to consider and acknowledge the wider social, economic and mental health consequences. Helping people with mental health support, cash or commodities and food, especially to vulnerable groups, can be necessary. For example, the projects provided key commodities, such as water and soap for handwashing, and masks to make sure that people could follow protective behavior. In every emergency, especially in the ones surrounded by a lot of uncertainties, finding the right way of addressing misinformation, by tracking rumors and collecting feedback from the community, to understand their perceptions and beliefs and answer to it with tailored communication strategies, has to have a major focus.
To stop the spread of the virus, it was necessary that the projects advocated for equal access to COVID-19 vaccines and supported the roll out of vaccine campaigns, especially in hard-to-reach areas. Supporting non-COVID health services, such as children's routine vaccinations that were disrupted by the pandemic response, was also essential, and will be of great importance during a future epidemic.
Epidemics can be controlled with simple steps like handwashing with soap. But long-term investments need to occur, to prevent the spread of diseases that are yet unknown. Investing in the water supply is one good example. These investments also need to be sustained in the long run. Investing in the capacity to anticipate and respond to epidemics at the local level is also important. Communities and local authorities have to be able to understand epidemic risk and put in epidemic preparedness action plans. In case of danger signs, they can react in time, preventing and controlling further spread of diseases. Epidemics start and end at the community level. Strengthening approaches that allow to engage with communities and local actors in epidemic preparedness and response is vital.

To find out more about the project, contact
Libertad Gonzales (lgonzales@redcross.nl) and Selam Seje (sseje@redcross.nl)
The Faces of Covid online report is based on the country reports provided by the Red Cross and Red Crescent National Societies.
2023 ©